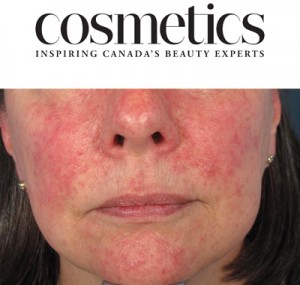
 If you find it tricky to distinguish between acne and rosacea, you’re not alone: Though they’re distinct skin conditions, requiring very different treatment approaches, they can sometimes appear with lookalike symptoms. For instance, papulopustular rosacea, a moderate form of the condition, typically shows up as persistent redness and pimple-like bumps.
If you find it tricky to distinguish between acne and rosacea, you’re not alone: Though they’re distinct skin conditions, requiring very different treatment approaches, they can sometimes appear with lookalike symptoms. For instance, papulopustular rosacea, a moderate form of the condition, typically shows up as persistent redness and pimple-like bumps.
Cosmetics Magazine asked Dr. Marcie Ulmer, Vancouver dermatologist and spokesperson for the Acne and Rosacea Society of Canada, how to differentiate rosacea from acne, and how to treat and prevent flare-ups.
They asked her several insightful questions, and then provided an excellent side-by-side rosacea/acne comparison with a full breakdown of symptoms for each condition, as well as an overview of treatment options, available following the questions below.
What are the main causes of rosacea, and who is at risk?
In some patients, there is a family history of rosacea and a genetic component; individuals with fair complexions of northern European descent tend to be more susceptible. Rosacea patients have an impaired skin barrier function and skin inflammation, and research is being done [on how] the vascular and nervous systems [are involved in the condition]. People with rosacea tend to flush easily and may have background redness and dilated blood vessels. They also tend to have a higher number of normal skin mites, which are possibly involved in the inflammation associated with rosacea. It often starts between the ages of 30 and 50, and affects more women than men.
Can rosacea be prevented?
There is no known way to prevent or cure rosacea, but it can be successfully managed.
How can rosacea best be treated?
[People with rosacea symptoms should] see a doctor first. A visit with a dermatologist may be necessary if the diagnosis is in question, or standard therapy is not effective. With the right diagnosis, there are many very effective treatments available. Flare-ups of rosacea can be minimized by avoiding known triggers such as spicy foods, hot beverages and alcohol, rigorous exercise, stress, excessive heat, certain cosmetics and sun exposure. Triggers are different for each person, so it is important to find out what an individual’s aggravating factors are. UV exposure is a common trigger, so it is recommended that people with rosacea use a minimum SPF 30 sunscreen daily.
Why is rosacea so often confused with acne?
Both acne and rosacea can present with red pimples, pustules and redness. While it is possible to experience both acne and rosacea simultaneously—and some medications do help both—it is important to have an accurate diagnosis to ensure appropriate treatment. [See Dr. Ulmer’s chart below for a rundown of the key differences.]
What is the main risk if rosacea is mistaken for acne?
If a patient with rosacea is mistakenly treated for acne, their skin can become quite inflamed and irritated. Rosacea patients tend to have sensitive skin in general, and adding an acne therapy can be very drying and irritating to their skin.
Is It Acne or Rosacea?
Vancouver dermatologist Dr. Marcie Ulmer breaks it down:
| SYMPTOMS | ACNE | ROSACEA |
| Who’s Affected | Most often teens; 1 in 5 women aged 20-50 | Mainly women aged 30-50 |
| Spots | Blackheads, whiteheads, pimples (pustules), red bumps (papules) and/or cysts | Pimples (pustules) and red bumps (papules)
There are no blackheads or whiteheads in the area where pimples have broken out |
| Redness | Red circles around inflamed pimples or within red bumps | Areas of permanent redness on the face, most often on the cheeks, nose, forehead or chin |
| Affected Areas | Face, neck and/or sometimes back or chest | Central face, especially on cheeks, nose, forehead or chin, and sometimes neck or chest |
| Blood Vessels | No | Tiny blood vessels visible |
| Flushing | No | Easy flushing and blushing |
| Eyes | Not affected | More than half of rosacea sufferers have eye symptoms—watery eyes, irritation, foreign body sensation, red lids or more serious disease |
| Pain | Some deep acne cysts can be very painful | Sometimes a burning sensation and skin sensitivity |
| Duration | Usually during the teen years
For some adults, into their 20s, 30s and even 40s |
A lifelong condition that starts in the late 20s or 30s |
| Family History | Almost everyone experiences some degree of acne at some point | 30 percent of rosacea patients have a close family member with the condition |
| Ethnicity | Affects people of all ethnicities | Affects mainly those of Celtic or northern European origin |
| Triggers | Tight headwear such as helmets; skin friction causing irritation; stress; and for some, consuming a high-glycemic diet or dairy | Exposure to sunlight; consuming alcohol, hot/spicy foods or hot drinks; stress; strenuous exercise; hot baths or showers; crowded spaces; cold and/or windy weather; and some topical products |
| Treatment Options | Over the counter: oil-free, gentle skincare; products containing salicylic acid and benzoyl peroxide
Prescription: multiple topical and oral medications are available; laser therapy can be beneficial for acne scars |
Over the counter: gentle skincare, camouflage makeup and sunscreen
Prescription: multiple topical and oral medications are available; laser therapy and intense pulsed light (IPL) can be beneficial for dilated blood vessels and redness |
| Outlook | Acne can be controlled with self-care and medical treatment if needed
Treatment has been shown to significantly improve the condition and improve a person’s outlook |
Although it cannot be cured, rosacea can be controlled with self-care and medical treatment if needed
Treatment has been shown to significantly improve the condition and improve a person’s outlook |
Please click here for the original posting on Cosmetics Magazine.